
Born With One Lung: The Diagnosis Doctors Almost Always Miss
There is a particular kind of silence that falls over a room when a diagnosis has no easy follow-up sentence. Pulmonary agenesis is that kind of diagnosis.
One or both lungs fail to develop entirely. Not underdeveloped. Not damaged. Simply absent. It sounds incompatible with life — and yet, some of these patients are sitting in clinics today, breathing with what they have, outliving every early prediction made about them.
I have seen both sides of that range. Here is what every family and clinician should understand.
What Is It — and How Rare?
Very early in pregnancy, before most mothers know they are pregnant, the lung buds fail to develop into bronchi, lung tissue, and blood vessels. The window closes. The lung never forms.
It occurs in roughly 34 per one million births. Most physicians will encounter it once in a career, if at all — and that unfamiliarity is precisely why it is so often missed.
_Two Forms. One Survivable_ yes it’s that bad
Unilateral pulmonary agenesis—one lung absent — is the survivable form. The remaining lung adapts, compensates, and in many cases carries a patient well into adulthood. Some are symptomatic from birth. Others are diagnosed years later, incidentally, during imaging for something else entirely.
Bilateral pulmonary agenesis— both lungs absent — is incompatible with life. Survival doesn’t rest in the hand of owner …solely lies with nature
Why It Keeps Getting Missed
This is where diagnostic errors cluster — and where they cause the most damage.
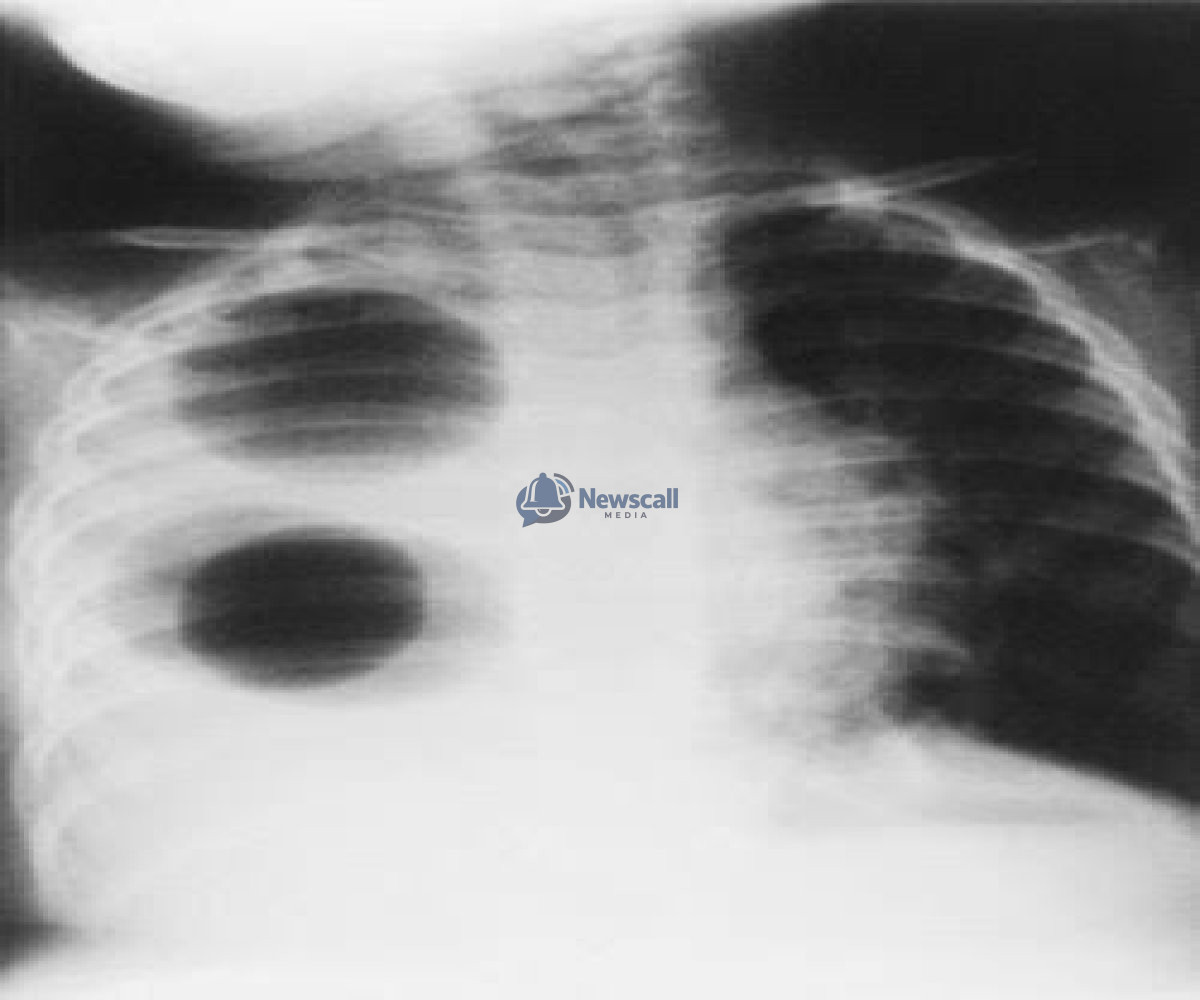
When one lung is absent, the heart and central chest structures shift toward the empty side, a finding called _mediastinal shift_. On a plain chest X-ray, this mimics two far more common conditions: complete lung collapse (atelectasis) or fluid around the lung (pleural effusion). Patients are treated for the wrong condition. Weeks pass. Sometimes months. By the time cross-sectional imaging is finally ordered, the family has already endured rounds of treatment that were never going to work. So hard to spill but double difficult to swallow
This is not a failure of intelligence. It is a failure of familiarity. And it is preventable.
A chest X-ray can raise suspicion. It cannot confirm the diagnosis. CT or MRI is required.
On imaging, atelectasis reveals a collapsed but present lung; pleural effusion shows compressing fluid. Pulmonary agenesis shows neither — no lung tissue at all. That absence is what makes the diagnosis.
Prognosis: The Honest Answer
Outcomes are genuinely variable — and I say that not as a clinical hedge, but because it is the most honest thing one can offer a family sitting across a desk, waiting for a number.
Three factors shape prognosis more than any other: the presence of associated cardiac defects, the development of pulmonary hypertension_(elevated pressure in the lung’s vessels), and the cumulative damage from repeated respiratory infections over time.
For patients with isolated unilateral agenesis and no major co-existing anomalies, survival into adulthood is achievable. Approximately half survive at least five years; many live ten, twenty, or more. Individual trajectories are genuinely difficult to predict — which is itself important for families to hear.
What Actually Makes a Difference
There is no intervention that restores an absent lung. Management is about protecting what exists.
Infection prevention is non-negotiable — the remaining lung carries the entire respiratory load, and serious infections are a direct threat to the only functional lung tissue the patient has. When pulmonary hypertension develops, the ain should be to improve vascular resistance and improve functional capacity. Pediatric pulmonology, cardiology, and thoracic surgery should be coordinating care — not operating in silos.
For a small subset, lung transplantation enters the conversation. The word lands heavily the first time it is spoken — and it should, because it is not a light option. Median post-transplant survival is approximately five years. Chronic lung allograft dysfunction— gradual rejection over time — remains the primary barrier to long-term success. Transplantation is a last resort, reserved for when all other options have been exhausted.
Three Things That Are Simply Not True
One missing lung means 50% capacity.”
The remaining lung compensates significantly through adaptation and hyperinflation. Function is not simply halved.
A chest X-ray is enough.”
It is not. Mediastinal shift convincingly mimics atelectasis and pleural effusion on plain imaging. CT or MRI is required.
“This is always fatal.”
It is not. With appropriate management and no severe co-existing anomalies, many patients achieve long-term survival.
For Families
No clinical summary prepares a family for what this diagnosis means in practice — the weight of every cold season, the uncertainty that never fully resolves.
What the data does not capture is that this condition can surprise you. There are patients living well beyond early estimates, whose outcomes were shaped as much by attentive care and early referral as by the diagnosis itself. I have seen it. The statistics are real — and so are the exceptions.
Early specialist referral changes what families are told, what is monitored, and what is caught before it becomes a crisis.
Do not wait.

Abiodun Oluwafemi
Copywriting, brandnaming, research. I deliver medical counseling and proper medical guidance .





